EPISODE · Mar 16, 2026 · 31 MIN
Cat Pits, Reddit Death Threats, and Stipulated Agreements
from The Information Exchange · host Brendan Keeler and Ryan Tucker
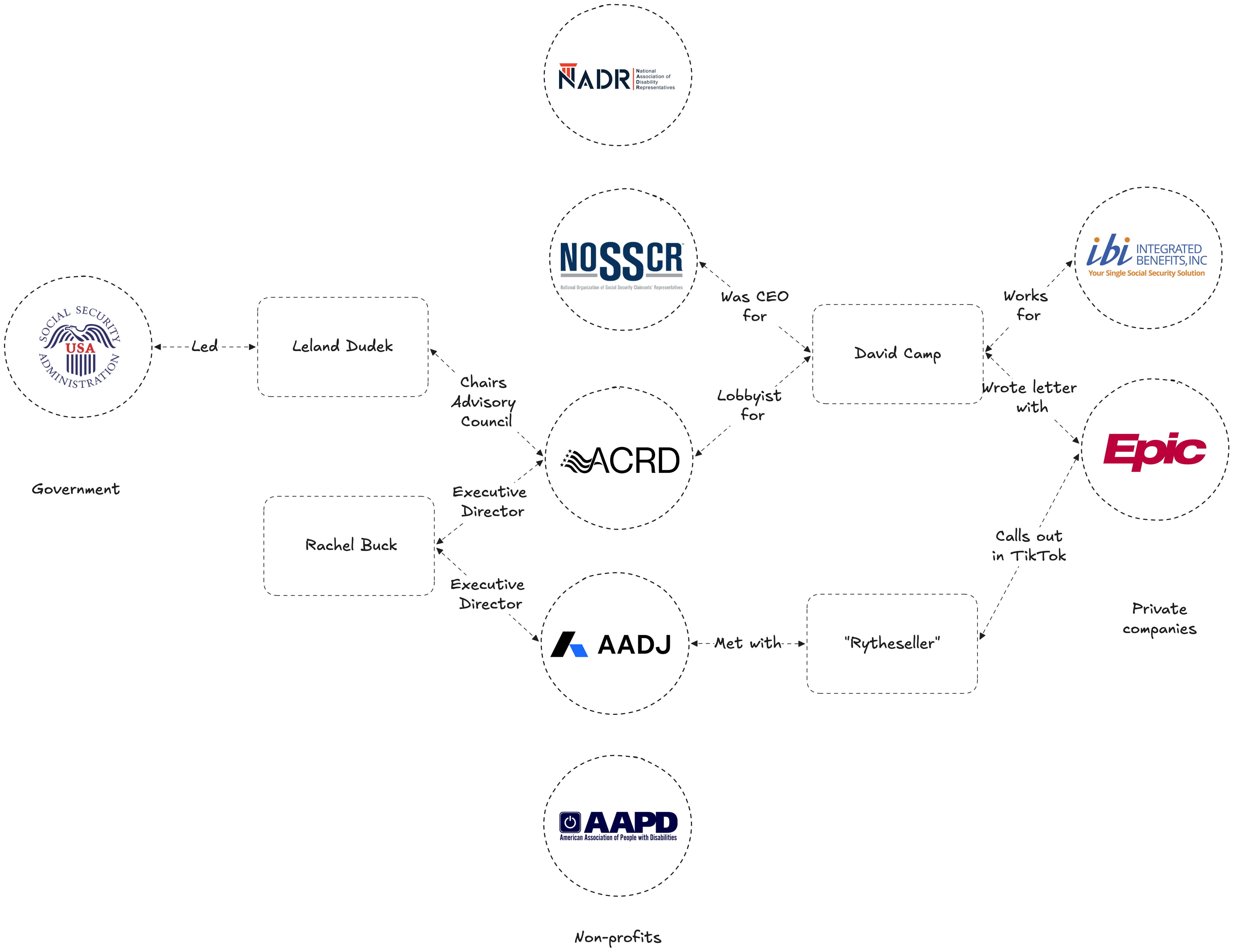
Healthcare’s biggest conference has come and gone, so the team is back (down a man or two) to bring you some updates there, as well as every twist and turn of a very busy week in the courts.* HIMSS 2026 felt smaller but more productive…and the sentiment was surprisingly pro-HIMSS over ViVE* AI headlined as expected, but the real conversations were about data normalization and cleanliness underneath the agentic hype* Epic subtly debuted Willow Pharmacy Network, a new “With the Patient at the Heart” product that could signal a long-term play against Surescripts* The American Association for Disability Justice filed antitrust and information blocking claims against Epic over MyChart’s fragmented login experience* A surprise stipulated agreement from GuardDog Telehealth reshapes the Epic v. Health Gorilla case ahead of April’s motion to dismiss hearing* Ryan recaps a guest lecture at Johns Hopkins and the malpractice risk thread that explains more about healthcare’s data reluctance than most people realizePlus we mentioned rumblings of a bonus class action lawsuit, which came true later that afternoon as Fox, Edward v. Epic, Beaudreau, Edgar v. Epic, and Banh, Priscilla v. Epic all kicked off. While on paper it’s not great for Epic, there’s potential upside if they’re able to consolidate effectively.Relevant Articles* Epic's AI announcements: The baseline announcements from Epic at HIMSS which were very AI focused* Introducing Copilot Health: Microsoft’s buzzy announcement of a consumer health product powered by HealthEx, paralleling ChatGPT Health and Claude Health* Epic Beyond the Provider Empire: This article explained Health Grid products and waxed hypothetical about a future pharmacy oriented product, which we saw at HIMSS via Willow Pharmacy Network* Down the Disability Data Rabbit Hole: The strange fruit of minot investigational journalism into a beef tallow influencer’s medical records videos, including one that targeted Epic* Ryan’s post on data quality: Pipes are only half the battle. As access becomes ubiquitous, it’s about what you do with it (if you even can).* AADJ v. Epic: The unexpected lawsuit that launched during HIMSS with disability advocates and patients claiming antitrust, information blocking, and disability violations, which explained Mr Beef Tallow Influencer above* Epic's TEFCA IAS plans: This details their MyChart Central / unified login plans, which seemingly contradict the AADJ claims* Epic v. Health Gorilla: GuardDog Rolls Over: The bombshell of one of the defendants in the Health Gorilla lawsuit turning tail and entering into consent by admitting various violations* Epic Lawsuit-ception: After recording Friday, the lawsuits we alluded to came to light as three separate templated class action lawsuits were filed against Epic for inappropriately disclosing PHI to Health Gorilla.Chapters* HIMSS Recap: Overall Impressions (00:00) - Brendan’s on-the-ground take from HIMSS in Vegas — attendance trends, booth culture, the cat pit, and general sentiment versus ViVE.* AI Announcements: From Chatbots to Agentic (02:48) - Epic’s Art/Penny/Emmy rollout, Microsoft’s patient access chatbot with HealthEx, Agent Factory, and the gap between clean demo environments and messy real-world data.* Data Normalization and the Infrastructure Layer (05:19) - The wave of companies tackling data cleansing, parsing, and augmentation as TEFCA and information blocking rules make data movement easier.* The Under the Radar Announcement of Epic’s Willow Pharmacy Network (06:16) - A new “With the Patient at the Heart” network product targeting specialty pharmacy workflows — and what it signals about Epic’s beachhead strategy into pharmacies and potentially e-prescriptions.* New Lawsuit: Disability Access and MyChart (09:07) - The American Association for Disability Justice files antitrust and information blocking claims against Epic over fragmented portal logins, plus analysis of why the legal claims face uphill battles.* TEFCA, IAS, and Health Tech Ecosystem Updates (16:23) - Kill the Clipboard demos, digital identity with CLEAR and ID.me, and Clover Health joining as the first payer in health information networks (plus the Wall Street Bets subplot).* Ryan’s Week: Teaching FHIR at Johns Hopkins (20:22) - A Q&A with grad students on interoperability trends, wearable data, and the signal-to-noise problem with smartwatch data flowing into clinical workflows.* Malpractice Risk as a Hidden Driver (22:28) - Why the fear of liability shapes provider attitudes toward data volume, RPM, AI summarization, and even HTI-5’s auditability certification debate.* Epic v. Health Gorilla: The GuardDog Settlement (26:35) - A surprise stipulated agreement from co-defendant GuardDog Telehealth changes the dynamics of the case, potentially undermining Health Gorilla’s procedural defenses ahead of the April hearing.TranscriptWe ran the transcript through an LLM to smooth it out. So it’s a rough approximation of the conversation (and in many cases significantly clearer than our rambling), but notably diverges from the word-by-word blows quite a bit.Ryan Tucker: So we are back with the Information Exchange — two out of the four players here, but we’re going to go strong. I would love to start with a HIMSS recap from you, Brendan. I was pretty busy myself on the other side of the country. Didn’t make it out to HIMSS. Saw some news, but I would love to hear your take. What happened?Brendan Keeler: Yeah, quite a lot. Have you been to HIMSS before? I don’t know if we’ve ever synced on this.Ryan Tucker: Yeah. So I went when I was with Epic, I think about two years in, and I was in the basement doing an Interop Showcase or whatever it was called, where I ran the same script I think 45 times in two days. So that was a very repetitive, not a great experience just in terms of personally needing to do the job there, but it was fun and Vegas was fun. It would be a very different experience now. I’ve been able to go to ViVE since then and things like that, but I haven’t been back since that one showcase.Brendan Keeler: You go to Vegas too many times and you’re in the Venetian over and over again, it just blurs the years. Booth working is different than sort of rogue agent parachuting in and having 12 meetings a day, which is the way that we typically operate when we go to HLTH and ViVE. You can more easily find ROI for certain companies if you’re setting up meetings, going and ad hoc meeting people — versus a booth that really is six figures or above as soon as you have something hanging from the ceiling.Our colleague Brad and I went out, had a ton of great meetings. Overall it felt a little smaller. Since the sale of HIMSS to Informa a couple of years ago, we’ve seen a contraction from 35,000 or whatever it is to 30. And I feel like it may have trended down — the booths were a little more spread out, it felt more spacious in terms of the throughways and stuff like that. There was all the requisite weirdness in terms of people going a little too far with marketing and putting stuff out there. There was one group that had a robot hand on their head that was going like this. That was probably the highlight of weirdness.But it was good. It was very productive. A lot of sentiment was “this is way better than ViVE,” which you don’t expect. They had a cat pit instead of a dog pit. So ViVE typically has all these puppies you can go play with, and they had kittens. I didn’t get a chance to do that, but it seemed pretty cool. They’re trying to be competitive with ViVE in that regard. Are you more of a cat or a dog person?Ryan Tucker: Definitely a dog person, but I would pet a cat.Brendan Keeler: Yeah, kittens are still cute, fluffy — anything to deal with the hangover of being in Vegas. But beyond that, what did we see? AI, all the things, right? Epic, if you look at all the press releases that went through CNBC and Modern Healthcare, it was just all Art and Penny and Emmy for Epic — their AI announcements. We had consumer-facing AI from Microsoft, which is interesting. That’s not particularly their slant versus some of these other companies, but they released in partnership with HealthEx their patient access and chatbot experience. So AI headlined, as you might expect.Ryan Tucker: Yeah. I mean, I think we see that universally all the time at this point, but that’s what I was seeing between meetings, checking on news. Epic, Amazon, Microsoft, Oracle, athenahealth — everyone had “here’s our take on AI.” Epic came out with Agent Factory. So I think we see the shift from general chatbot or LLM AI to agentic AI becoming prevalent.I did put a post on LinkedIn about this. I think there’s a big difference between what you can show at a HIMSS showcase when you have a very clean data environment and a simple workflow to say, “Wow, look at what this can do,” versus AI in the real world — especially with health system data where we know the pipes might be there, interoperability might be working in terms of connecting from place to place, but there’s a lot of bad data out there.The utilization of that data is what’s becoming important. I think especially with agentic use, being able to have a provider just type in something from a prompt and pull up the record that they’re concerned with — we need to have a lot of good data classification, normalization, cleansing of the data that comes in. So I guess I’m wondering, was there any level deeper? Starting on the Care Everywhere team at Epic, we were obsessed with raw number record exchange first. And then it slid toward how we’re actually using the data once it got there. Now with AI, do you see that start to shift — or not yet — where it’s “AI is here, but now how do we actually start to use it”?Brendan Keeler: Totally. Brad and I had maybe four straight conversations where some slant of it was data normalization, augmentation, cleanliness. And sometimes that was using an LLM — off the shelf, commercial off the shelf like OpenAI or something. But then other tools using machine learning or their own models or whatever it might be to be more healthcare specific and to get to a higher accuracy rate.So certainly, as we have Carequality and TEFCA and information blocking — all these things mean that data movement is much more accessible. The cleaning of it, the parsing of it from those data sources and others like fax — there’s a ton of infrastructural companies vying to make their play in that space. So certainly prevalent.I think the other thing, the off-the-radar announcement that I can’t even find on the internet right now — at the Epic booth, looking at “With the Patient at the Heart,” the Health Grid products, their network-based products, there was the addition of a new one which I had never seen before: Willow Pharmacy Network. It was something around specialty pharmacy workflows to start, but much like Epic Payer Platform isn’t taking on clearinghouse roles but rather clinical data exchange — so an adjacent payer functionality that gives them a beachhead to sell into payers, a beachhead to potentially go do eligibility and claims down the line.That business strategy is now being applied to pharmacies, where they already have a system of record they can sell — Willow Ambulatory — and potentially after they build this network product and get deployment, perhaps they can go do e-prescriptions. Perhaps they can do other workflows and take on Surescripts. It’s something that I posited in an article a couple of years ago, but it’s interesting to see it play out in some fashion. I’ll be excited when it’s actually on the website, when I can see it anywhere else and we can learn more details. But that was my “beneath the AI radar” announcement.Ryan Tucker: Yeah, that’s really interesting. And I think you’re right — I didn’t see news around that. So you brought it up as a networking-type side product. Are they actually thinking of the movement of data, analogous to Surescripts, or is it more the workflow around specialty medication management — prior authorization, things like that?Brendan Keeler: It was distinctly in the Health Grid. Now I keep calling it Health Grid because it’s a better name than “With the Patient at the Heart.” But the “With the Patient at the Heart” products: Epic Payer Platform, Discovery for clinical trials, forgetting some of the other ones that are in there — they’re all network products. They sell to non-provider organizations and say, “We can help you integrate with our provider base more seamlessly using these products.”Epic Payer Platform is certainly the buzziest, most well-known of those, but Aura being for labs and medical device companies, “Supplies on Time” being for medical device manufacturers — all of those are network-based products that have the dual strategic purpose of giving them sales distribution to a new customer type, and then from there, they can sell systems of record to those customer types. Potentially Tapestry for payers, ERP to supply manufacturers, hypothetically Willow Ambulatory to pharmacies.It was visually lumped with those products, which is suggestive of the network product. And then from some late, fairly hungover discussion with the team there, they mentioned it being some network-based product for specialty medication workflows.Ryan Tucker: That’d be interesting to see. I mean, Epic is everywhere all the time. What are they not getting into at this point?Brendan Keeler: Well, what they’re not getting into is avoiding lawsuits, which is another — the Rule of Conferences held true. So last week we did some spelunking through TikTok and found this interesting beef tallow influencer that was talking about medical record release. And we’re like, what is going on here with this American Association for Disability Justice nonprofit?You and I had talked about it last week with Brad and others — there was just no resolution. Well, now we have more clarity because during the conference, the Rule of Conferences held true, and that group, that nonprofit, launched a new lawsuit alleging antitrust, information blocking, and violation of disability-related laws as claims against Epic in regards to MyChart not having a single login.That is how patient portals work generally across most EHRs. But suffice to say there’s frustration in the industry — in the disability industry that helps with claims to Social Security — that they’re still unable to get medical records in a timely fashion. That frustration is real. The claims are going to be challenging for the plaintiffs just because — again, not a lawyer — but looking at them, for the antitrust claims, the market definition they state is a 40% market share, which is typically quite low for antitrust claims. They don’t properly assert in my mind some of the implications that are necessary. But we’ll see.For information blocking in particular, when we’ve seen successful information blocking claims, they’ve used what you might call state tort hooks — where they’re not saying “This is the law, information blocking law was broken, I can sue you,” because that would entail the private right of action to be detailed by Congress. Instead, they say, “Because you broke information blocking federal law, you’ve broken state tort law — unfair competition law and things like that.” You’re actually suing under breaking California’s unfair competition law or something of that nature.That’s not what they do here. They just say “You broke information blocking law. This is a claim against you.” I don’t think that’ll hold up, given the lack of private right of action. Imagine Epic will push back there.So yeah, it’s an interesting case and it just shows that there are still many problems to be solved in terms of interoperability and where we need digital, ubiquitous digital exchange in as frictionless a pattern as possible — to help disabled people get their Social Security benefits, to help all the other underserved use cases that currently people are trying to funnel through the treatment purpose of use.Ryan Tucker: It’s a really interesting space. You said you’re not a lawyer. I’m even further away from legal understanding on that spectrum. You bring up the term “torts” and I get a little hungry because I think of tortas. I read your article covering this.Obviously they make a lot of claims, and I agree that there is well-founded frustration when it comes to the fragmentation of this information, the inability to easily get this when trying to make a disability claim. You brought up the patient portal side — that they’re not having just one login to MyChart, which I think actually Epic is working on something like that, to help with accessing all of your MyCharts no matter which Epic-specific health system you’re at.But I was just curious — that fragmentation is not due to Epic. And I think we understand that pretty well. There are obviously multiple Epic and non-Epic health systems. We don’t have a federally mandated “one record to rule them all” within the country. So I think a lot of that is not Epic’s issue, and it’s certainly not an only-Epic issue. I don’t know if this is a case of going after the biggest player in the space because it’s a problem all the way down. I’m just trying to understand — is Epic really responsible? And if they are, then I feel like all the EHRs are responsible. I’m just kind of confused about how this would play out.Brendan Keeler: A couple of thoughts here. One is intuition — the way we intuit what is right or wrong, ethics, things like that. Those are all different. The law may be a full Venn diagram overlap with our intuition, or it may be zero Venn diagram overlap. So we’ll talk more about intuition. I gave some non-lawyer legal perspectives on what might happen based on analysis of those claims.But you’re right. The architecture of Epic and Cerner and many of these others is that they’re sold to hospitals, sold to institutions, and those institutions want the agency to own and control and set up the software. Part of that is their patient portal, which they brand and configure and make changes to.That historical baggage has been true. The lawsuit mentions using TEFCA Individual Access Services and, when doing so, being unable to retrieve data from the Epic sites because of portal credentials. And that is a current function of how Epic has architected their Individual Access Services that other EHRs participating today have not.To your point, Epic has announced — and they have on their TEFCA website — that by the end of the year they’re going to have MyChart Central and more single unified login, as well as the CMS-aligned networks under the CMS Health Tech Ecosystem pushing Epic and other EHRs to go further in easing authentication and removing that double authentication step.But Epic’s choices here are not by and large them saying top down, “This is what it will be” to their health systems. These health systems have strong privacy considerations that they’re thinking about. There were rumors — I’ve yet to find this online — but there were rumors that there’s another class action lawsuit against Epic and hospitals in some state courts claiming they’ve released PHI inappropriately in violation of HIPAA. So patients suing Epic and/or hospitals for HIPAA breach.That risk is what underpins, or at least is stated to underpin, a lot of the behaviors of the health systems and of Epic to serve those health systems. It’s an interesting, testy time, and we’ll see where this claim goes. If there’s any positive for the plaintiffs, the jurisdiction — Western Texas, so I think it’s Austin — where that locus is, is pretty favorable to pushing the limits on some tech-forward lawsuits. I think that was a strategic choice to file there.Ryan Tucker: Definitely. So you mentioned IAS — Individual Access Services. I think the end goal that we’d love to see, and we understand the technical logistics of how difficult this might be, is something like an application on your phone where you’re able to see “these entities have my health data” and you have levers that control access, can transfer access, those types of things. We’re a long way away from there.I was just curious — you went over the announcements with HIMSS. Anything to report in terms of the Health Tech Ecosystem and some of the main initiatives, which included patient access and Kill the Clipboard?Brendan Keeler: There were awesome demos. Participants in terms of eClinicalWorks — either for the Healow product or maybe just the EHR — alongside other parties showing that Kill the Clipboard exchange. A lot of interest and discussion of digital identity — CLEAR and ID.me as the two main credentialed service providers, but potentially more entering and certifying in order to serve the TEFCA Individual Access Services and CMS-aligned network ecosystems.And then we had Clover Health join last week as a payer — the first payer to really participate in health information networks. They’re just responding to start to Individual Access Services, but then treatment in some short order once they ascertain that the treatment queryers can actually store FHIR Explanation of Benefit bundles. That’s a new payload type that if they just throw it over the wall, probably some EHRs and other queryers will bomb out. So really cool leadership by Clover in doing this.But man, that post really cooked on LinkedIn, because the Wall Street Bets community — they love Clover Health as a public stock. So anytime you put “Clover Health,” like, “Have you read my analysis of XYZ?” I’m like, “But sir, this is a Wendy’s.”Ryan Tucker: They want Clover to go to the moon.Brendan Keeler: When the CMS RFI — Request for Information — last summer was going through the comments, I’m reading, I like to read the comments because I’m a dork. And as you see over and over again in this broad, expansive “What should CMS do in terms of tech? What should ASTP do in terms of tech in this administration?” — that was sort of the thrust of the RFI. There’s just comment after comment like, “Well, they should just buy and mandate Clover Health.” And I’m like, what’s going on here?Talked to some people over at Clover and they’re like, “Oh, no — it’s Wall Street Bets from Reddit.” So I went to Reddit and found a thread where somebody’s like, “Hey, there’s this new question from the CMS, we gotta go hype Clover Health because then they’ll go buy Clover Health.” And so you have 20, 30, 40 comments of this nature, this comment campaign.I posted about it and then I’ve never received more death threats than from the community saying, “You don’t understand the magic and the power.” And I’m like, I do. I know them very well from working with them over the years and I’m friendly with them. So every regulatory thing — HTI-5, CMS RFI — you always get some interesting, unexpected comment campaigns. But that was one where I’m like, man, that’s an intersect I was not expecting to have — the SPAC crowd from Chamath’s world come on over and get involved in a CMS RFI.Ryan Tucker: The wonderful and horrifying discourse of the greater internet there.Brendan Keeler: Anytime you add anonymity of any kind to social media, you start to get some really interesting outcomes. So yeah, that’s the rabbit hole we go down from HIMSS. But you weren’t at HIMSS. Maybe you want to tell the audience a little bit about what you worked on, because I thought it was interesting.Ryan Tucker: Yeah, definitely an interesting, busy week. One of the main highlights was Monday night — Joe Mercado from Arcadia and CareJourney invited me to speak with his class at Johns Hopkins, which is a school of medicine class that has a mixture of grad students in public health and different areas. It was a class on FHIR. Basically a Q&A for about an hour and 15 minutes, and it was just great to see about 15 students and their different perspectives, the questions that they asked. It was a joy to be there.But really, I think a lot of the things we talked about coming from HIMSS were top of their mind. They wanted to understand trends over time in the interop space. And we talked about how the record exchange then turned into data usage. They brought up wearable technology — not like blood pressure cuffs or pulse oximeters, but they’re very interested in smartwatches. There was a cardiologist there and she would like to understand how to get the data from a smartwatch to help with her practice.I think there’s a thread that could be connected to the AI side we were talking about, where there’s a signal-to-noise problem. Yes, a cardiologist may be interested in trending over time of what your heart rate looks like or within a particular stress event. But if you include every single moment of your life within that smartwatch’s data and you send that into a chart, the provider is going to be overwhelmed. There’s that signal-to-noise ratio — they’re not going to know what to do.Very similar when it comes to AI usage and prompting. If you have bad data, if you have too much that you’re not able to properly classify, sort through, search through — it doesn’t matter if you have all the data in the world. It needs to be usable.Brendan Keeler: That’s one part of it, but a lot of times when I’m looking at dysfunctions in healthcare, particularly in US healthcare, you look and you squint and you peel it back — malpractice risk is generally one of those big ones. If you start to peel back “why were they so cagey about what they said back to me,” so many times that behavior comes from the risk of malpractice.Certainly, dumping a bunch of cardiology data into a chart has some risk of “they don’t read it in time, something happens, and there’s a lawsuit.” That’s a common trope for why we don’t want all the RPM data back in the chart. And as a technologist, I’m like, we can have AI summarization, we can have alerting — there are ways to solve for it versus the Luddite “just don’t even give it to me!” Healthcare organizations should be data hungry to better care and have broader insights. And if the problem is the volume of it, well, let’s build the tools to distill it down appropriately. That’s my technologist view on it.Ryan Tucker: I’ve never really thought about that point around malpractice. You’re right — if there’s so much auditing available in the chart specifically for this, the more data they’re presented, the more they’re theoretically responsible for. And so the higher risk.That’s really interesting — we keep claiming we want more and more data. And then how does that play into when they didn’t see the source data, they only saw the AI summary, and things like that. That’s a fascinating thread to pull on that I really hadn’t thought about before.I have a lot of family in medicine. My wife’s a nurse, but I have an aunt and uncle who are like a real power couple — my uncle’s an ophthalmologist and my aunt’s an electrophysiologist. I love talking to them at family gatherings because I’m the one working in health IT. She has a practice where she uses a few different EHRs and it’s needing to chart constantly — we know about the pajama time and things like that.And then my uncle, who’s in ophthalmology, stayed away from it for as long as possible. They were a specialty that was able to stay on paper until very recently. He purposely owned his practice and said, “I don’t want to deal with this because I see my wife every weekend charting.” Basically, ignorance is bliss when it comes to that.That plays a big role too. I think he was narrowing his scope of responsibility also. It was more of the burden aspect he was trying to stay away from. But that’s such a good point — can a provider be held responsible to all this data that’s thrown at them? We need to make tools that make that easier to distinguish, but I really hadn’t thought about that before.Brendan Keeler: Everything is about lawsuits in America if you actually think about it too much. Even HTI-5 — I forget if we talked about it on a previous episode — but HTI-5 comments, the comment campaign for HTI-5 was just a big law firm push. All these law firms said, “Wait a minute, you’re removing certification criteria for auditability?” — that when somebody types in a note, it’s immutably stored, that something was written. Because if later something happens and there’s a malpractice lawsuit, if they can go back and edit that note to make it look like they were right, they could fudge things to get around it.When the ASTP said “Let’s get rid of auditability,” all these law firms who deal with that were like, “No, no, no, no.” This is the one good criteria — in a very selfish way for their own businesses. But in a way, there were poignant stories that some of these letters had about what they’ve seen, the realities of what they’ve seen shady doctors do. So — lawsuits, lawsuits as far as the eye can see.Ryan Tucker: Yeah, that’s probably a good way to sum it up. That must cover it for the week.Brendan Keeler: Well, it turns out — one more lawsuit. So yeah, just this morning we saw a very unexpected development in the Epic versus Health Gorilla case.In January, following the Rule of Conferences at JPM, we saw Epic sue Health Gorilla and a number of co-defendants, alleging that there was fraud. Epic was joined by Reid Health and Trinity Health and a number of health systems stating that these groups were using the health information networks to pull data claiming treatment, but really for mass tort purposes — identification of mass plaintiff lawsuits for PFAS exposure and things of that nature.We saw motions to dismiss a few weeks ago from Health Gorilla, from Ravilla Med, some of the defendants, that I thought were quite well done and articulate in the procedural angle of it — saying, “Hey, there is a process within TEFCA and Carequality to resolve these things that should be followed. And the only exception to that process is for preliminary injunction — if you need to move so fast to get relief, then okay, you can go around the internal processes of these trust networks.” And there was no preliminary injunction filed in the court case as far as we could see. So it’s like, all right, maybe Health Gorilla and RavillaMed have a point here.But a few of the other defendants were quite quiet. And now we know why — at least one of them was. This GuardDog Telehealth has a stipulated agreement now. They’ve settled with Epic by admitting to a number of things they’ve done wrong and potentially their counterparties as defendants have done wrong. What they say doesn’t mean it is truth — that needs to be proven in a court of law — but it is not great for the other defendants that they now have this on the record from GuardDog.That changes the dynamic of the case because it really favors Epic, obviously. It now allows them to potentially pick off other defendants and pit them against one another. Particularly Unit 387 is directly named by GuardDog in the allegations in this document. And there’s a preliminary injunctive element to this agreement that now may satisfy some of the procedural concerns.So a fairly deft update by Epic that changes the contours of this case quite a bit and just puts a pin on a very wild HIMSS week.Ryan Tucker: Definitely a lot going on. It’s such a weird one for me personally because there’s gotta be a very small crowd that has past employment history at both Epic and Health Gorilla. And I am one of those. So it’s difficult to comment on publicly.It seems like GuardDog coming out with this — the more procedural reply that Health Gorilla was bringing up last week, which you said does have some validity in terms of how TEFCA and the processes were supposed to work — it seems like that doesn’t help them, right? That’s going to be tough for them now because GuardDog is basically pushing this forward?Brendan Keeler: I think the next update we’ll see is the hearing on the motion to dismiss in April. That will be the big one. There might be some other briefs and stuff in the interim, but yeah, fascinating to see what counter move Quinn Emanuel — who represents Health Gorilla — might do to this. Could potentially maybe still push on it: “Well, that you didn’t actually do a preliminary injunction” or something in that procedural bent, or fall back to some of their other defenses they had in their motion to dismiss. In contrast to the RavillaMed motion to dismiss, the Health Gorilla and Quinn Emanuel motion to dismiss had a lot of other, more substantive arguments to fall back on. So yeah, we shall see.Ryan Tucker: We’ll see what happens in April and we’ll see if it’s a slower week next week. This was packed.Brendan Keeler: All right. Rock and roll. Get full access to Health API Guy at healthapiguy.substack.com/subscribe
NOW PLAYING
Cat Pits, Reddit Death Threats, and Stipulated Agreements
No transcript for this episode yet
Similar Episodes
Mar 26, 2026 ·1m
Mar 19, 2026 ·34m
Feb 18, 2026 ·11m
Feb 11, 2026 ·45m