EPISODE · Aug 25, 2025 · 7 MIN
📝 “How Do You Manage Chest Pain & Dyspnea Post-Op IV Sedation?”
from Dr. Gallagher's Podcast · host Brendan Gallagher, DDS
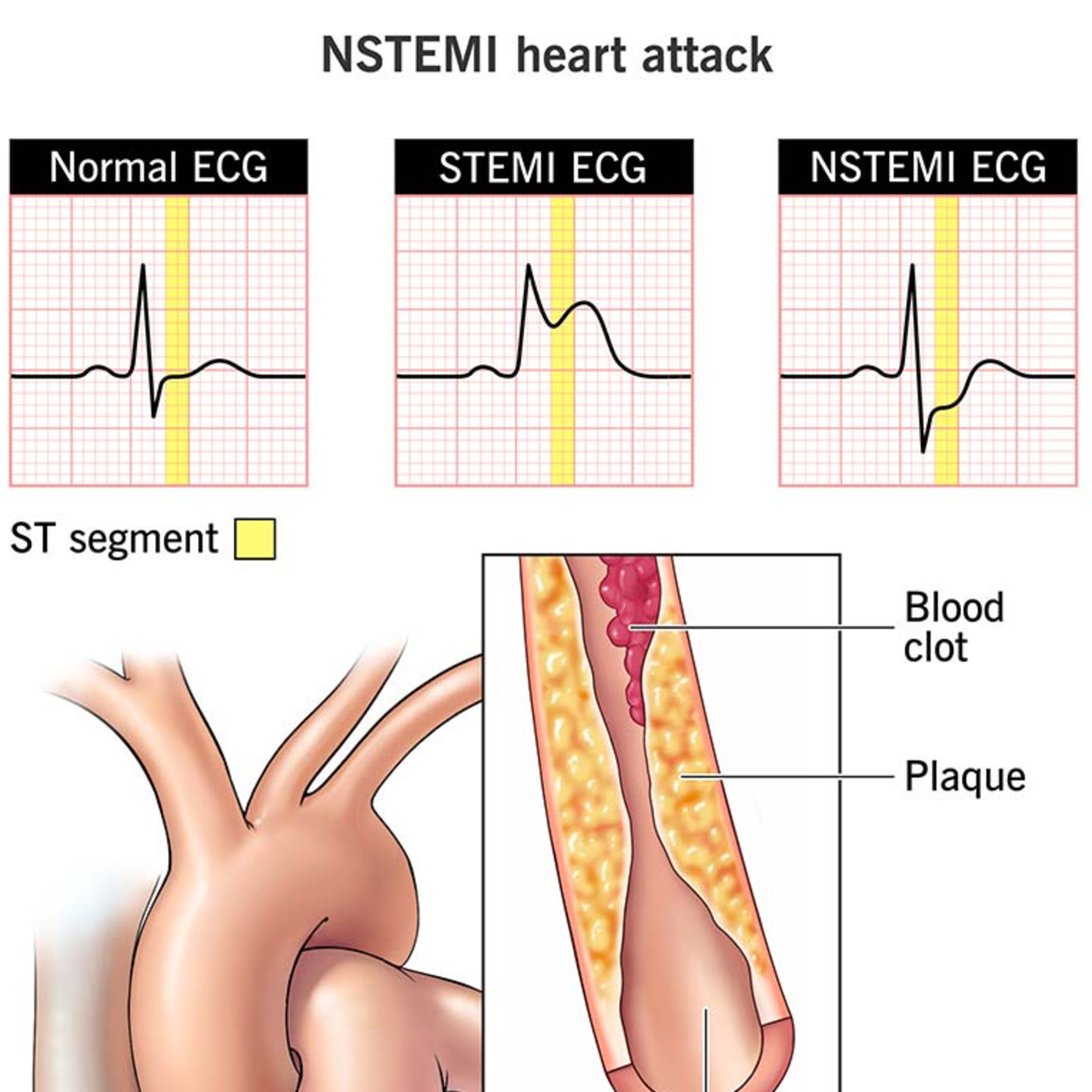
Quick Review #284 - #anesthesia #sedation #surgery #doctorgallagher #oralsurgery #oralsurgeon #omfs #dentist #dentistry - 8.25.25Post-operative chest pain and shortness of breath in a patient with hypertension undergoing IV sedation includes a differential diagnosis: myocardial infarction (MI), pulmonary embolism (PE), pneumothorax, and aspiration/airway compromise. Recognizing which diagnosis to rule out first is critical.Step 1: Initial AssessmentImmediately stop all activity, reassess ABCs (airway, breathing, circulation), apply 100% oxygen, and place the patient on full monitoring (ECG, SpO₂, BP). Chest pain with dyspnea must be treated as a presumed cardiac event until proven otherwise.Step 2: Prioritizing Differential• MI/ACS is the most urgent to exclude. A hypertensive middle-aged male is high risk. Acute chest pain and dyspnea strongly suggest ischemia. Perform an ECG first, looking for ST elevations, T wave inversions, or new Q waves. Administer chewable aspirin (325 mg) if no bleeding risk, and consider sublingual nitroglycerin (0.4 mg) only if systolic BP >90 mmHg. Call EMS immediately — definitive management requires hospital transfer and possible reperfusion therapy.• Pulmonary Embolism also presents with acute dyspnea and pleuritic chest pain, often post-op. Tachycardia, hypoxemia, and anxiety raise suspicion. However, diagnosis requires imaging (CT angiogram) not available in the office, making supportive O₂ and EMS transfer the main interventions.• Pneumothorax can follow PPV or barotrauma. Signs include unilateral chest pain, absent breath sounds, and hypotension if tension physiology develops. Requires urgent O₂, EMS transfer, and if crashing, needle decompression.• Aspiration/airway compromise is also possible, especially in sedation. Coughing, wheezing, or stridor point toward this. Immediate suctioning, airway maneuvers, and PPV with 100% O₂ are essential.Step 3: Key Learning PointThe most immediate diagnosis to rule out is MI because it is both common and most rapidly fatal. The first test is ECG — fast, accessible, and diagnostic. PE, pneumothorax, and aspiration remain high-yield considerations, but they are second-line in acute triage.References:1. Cleveland Clinic. (2023). NSTEMI: Non-ST-elevation myocardial infarction (heart attack). Cleveland Clinic.2. Miloro, M., Ghali, G. E., Larsen, P. E., & Waite, P. (2022). Peterson’s Principles of Oral and Maxillofacial Surgery (4th ed.). Springer.3. Abubaker, A. O., Lam, D., & Benson, K. (2016). Oral and Maxillofacial Surgery Secrets (3rd ed.). Elsevier.4. ChatGPT.2025.#podcast #dentalpodcast #doctor #dentist #dentistry #oralsurgery #dental #dentalschool #dentalstudent #dentistlife #oralsurgeon #doctorgallagher
What this episode covers
Quick Review #284 - #anesthesia #sedation #surgery #doctorgallagher #oralsurgery #oralsurgeon #omfs #dentist #dentistry - 8.25.25Post-operative chest pain and shortness of breath in a patient with hypertension undergoing IV sedation includes a differential diagnosis: myocardial infarction (MI), pulmonary embolism (PE), pneumothorax, and aspiration/airway compromise. Recognizing which diagnosis to rule out first is critical.Step 1: Initial AssessmentImmediately stop all activity, reassess ABCs (airway, breathing, circulation), apply 100% oxygen, and place the patient on full monitoring (ECG, SpO₂, BP). Chest pain with dyspnea must be treated as a presumed cardiac event until proven otherwise.Step 2: Prioritizing Differential• MI/ACS is the most urgent to exclude. A hypertensive middle-aged male is high risk. Acute chest pain and dyspnea strongly suggest ischemia. Perform an ECG first, looking for ST elevations, T wave inversions, or new Q waves. Administer chewable aspirin (325 mg) if no bleeding risk, and consider sublingual nitroglycerin (0.4 mg) only if systolic BP >90 mmHg. Call EMS immediately — definitive management requires hospital transfer and possible reperfusion therapy.• Pulmonary Embolism also presents with acute dyspnea and pleuritic chest pain, often post-op. Tachycardia, hypoxemia, and anxiety raise suspicion. However, diagnosis requires imaging (CT angiogram) not available in the office, making supportive O₂ and EMS transfer the main interventions.• Pneumothorax can follow PPV or barotrauma. Signs include unilateral chest pain, absent breath sounds, and hypotension if tension physiology develops. Requires urgent O₂, EMS transfer, and if crashing, needle decompression.• Aspiration/airway compromise is also possible, especially in sedation. Coughing, wheezing, or stridor point toward this. Immediate suctioning, airway maneuvers, and PPV with 100% O₂ are essential.Step 3: Key Learning PointThe most immediate diagnosis to rule out is MI because it is both common and most rapidly fatal. The first test is ECG — fast, accessible, and diagnostic. PE, pneumothorax, and aspiration remain high-yield considerations, but they are second-line in acute triage.References:1. Cleveland Clinic. (2023). NSTEMI: Non-ST-elevation myocardial infarction (heart attack). Cleveland Clinic.2. Miloro, M., Ghali, G. E., Larsen, P. E., & Waite, P. (2022). Peterson’s Principles of Oral and Maxillofacial Surgery (4th ed.). Springer.3. Abubaker, A. O., Lam, D., & Benson, K. (2016). Oral and Maxillofacial Surgery Secrets (3rd ed.). Elsevier.4. ChatGPT.2025.#podcast #dentalpodcast #doctor #dentist #dentistry #oralsurgery #dental #dentalschool #dentalstudent #dentistlife #oralsurgeon #doctorgallagher
NOW PLAYING
📝 “How Do You Manage Chest Pain & Dyspnea Post-Op IV Sedation?”
No transcript for this episode yet
Similar Episodes
Dec 5, 2025 ·50m
Oct 9, 2025 ·33m
Oct 3, 2025 ·40m
Sep 11, 2025 ·31m
Aug 27, 2025 ·39m
Aug 18, 2025 ·54m