EPISODE · Nov 17, 2022 · 12 MIN
Ultrasound of Acute Appendicitis
from Radiology Lectures | Radquarters · host Daniel J. Kowal, MD
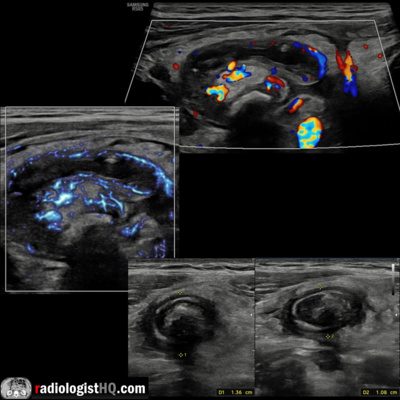
In this radiology lecture, we review the ultrasound appearance of acute appendicitis with three unique cases! Key teaching points include: Ultrasound is the first-line imaging modality in pediatric and pregnant patients due to lack of ionizing radiation: Sensitivity/specificity approximately 80%. Technique: Linear transducer with graded compression at site of maximal tenderness using gradual increased pressure to displace normal bowel gas. Inflamed appendix appears as a noncompressible, blind-ending tubular structure arising from cecum. Outer appendiceal diameter with compression: Less than 6 mm almost always normal, 6-8 mm borderline, greater than 8 mm highly suspicious. Thickened appendiceal wall (greater than 2 mm). Wall hyperemia: “Dot flow” normal, continuous linear/curvilinear flow highly suspicious. Increased echogenicity and expansion of peri-appendiceal fat due to infiltration by inflammatory cells and edema. Hyperechoic appendicolith with posterior acoustic shadowing supportive. Identify terminal ileum separate from appendix to differentiate from ileitis, Meckel’s diverticulum, or other small bowel abnormality. Appendix does not exhibit peristalsis. Right lower quadrant free fluid and lymphadenopathy supportive, but nonspecific in isolation. Loss of wall stratification suspicious for necrotic/gangrenous appendicitis, and color Doppler flow may be absent. Gas in appendix appears as dirty shadowing and ring-down artifact. Intraluminal gas sometimes helpful to exclude appendicitis, but can also be seen with gangrenous complication. Peri-appendiceal gas-containing collections highly suspicious for perforation. CT may be needed for clarification. References: Madhuripan N, Jawahar A, Jeffrey RB, Olcott EW. The Borderline-Size Appendix: Grayscale, Color Doppler, and Spectral Doppler Findings That Improve Specificity for the Sonographic Diagnosis of Acute Appendicitis. Ultrasound Q. 2020;36(4):314-320. Fallon SC, Orth RC, Guillerman RP, et al. Development and validation of an ultrasound scoring system for children with suspected acute appendicitis. Pediatr Radiol. 2015;45(13):1945-1952. To learn more about the Samsung RS85 Prestige ultrasound system, please visit: https://www.bostonimaging.com/rs85-prestige-ultrasound-system-4 Click the YouTube Community tab or follow on social media for bonus teaching material posted throughout the week! Website: https://radquarters.com/ Instagram: https://www.instagram.com/radquarters/ Facebook: https://www.facebook.com/radquarters/ Twitter: https://twitter.com/radquarters Reddit: https://www.reddit.com/user/radiologistHQ/
What this episode covers
In this radiology lecture, we review the ultrasound appearance of acute appendicitis with three unique cases! Key teaching points include: Ultrasound is the first-line imaging modality in pediatric and pregnant patients due to lack of ionizing radiation: Sensitivity/specificity approximately 80%. Technique: Linear transducer with graded compression at site of maximal tenderness using gradual increased pressure to displace normal bowel gas. Inflamed appendix appears as a noncompressible, blind-ending tubular structure arising from cecum. Outer appendiceal diameter with compression: Less than 6 mm almost always normal, 6-8 mm borderline, greater than 8 mm highly suspicious. Thickened appendiceal wall (greater than 2 mm). Wall hyperemia: “Dot flow” normal, continuous linear/curvilinear flow highly suspicious. Increased echogenicity and expansion of peri-appendiceal fat due to infiltration by inflammatory cells and edema. Hyperechoic appendicolith with posterior acoustic shadowing supportive. Identify terminal ileum separate from appendix to differentiate from ileitis, Meckel’s diverticulum, or other small bowel abnormality. Appendix does not exhibit peristalsis. Right lower quadrant free fluid and lymphadenopathy supportive, but nonspecific in isolation. Loss of wall stratification suspicious for necrotic/gangrenous appendicitis, and color Doppler flow may be absent. Gas in appendix appears as dirty shadowing and ring-down artifact. Intraluminal gas sometimes helpful to exclude appendicitis, but can also be seen with gangrenous complication. Peri-appendiceal gas-containing collections highly suspicious for perforation. CT may be needed for clarification. References: Madhuripan N, Jawahar A, Jeffrey RB, Olcott EW. The Borderline-Size Appendix: Grayscale, Color Doppler, and Spectral Doppler Findings That Improve Specificity for the Sonographic Diagnosis of Acute Appendicitis. Ultrasound Q. 2020;36(4):314-320. Fallon SC, Orth RC, Guillerman RP, et al. Development and validation of an ultrasound scoring system for children with suspected acute appendicitis. Pediatr Radiol. 2015;45(13):1945-1952. To learn more about the Samsung RS85 Prestige ultrasound system, please visit: https://www.bostonimaging.com/rs85-prestige-ultrasound-system-4 Click the YouTube Community tab or follow on social media for bonus teaching material posted throughout the week! Website: https://radquarters.com/ Instagram: https://www.instagram.com/radquarters/ Facebook: https://www.facebook.com/radquarters/ Twitter: https://twitter.com/radquarters Reddit: https://www.reddit.com/user/radiologistHQ/
NOW PLAYING
Ultrasound of Acute Appendicitis
No transcript for this episode yet
Similar Episodes
May 31, 2026 ·25m
May 31, 2026 ·30m
May 31, 2026 ·57m
May 31, 2026 ·32m
May 31, 2026 ·29m
May 31, 2026 ·37m