EPISODE · Dec 28, 2023 · 4 MIN
“What are the Types of NOE (Naso-orbitoethmoid) Fractures and How To Repair Them?”
from Dr. Gallagher's Podcast · host Brendan Gallagher, DDS
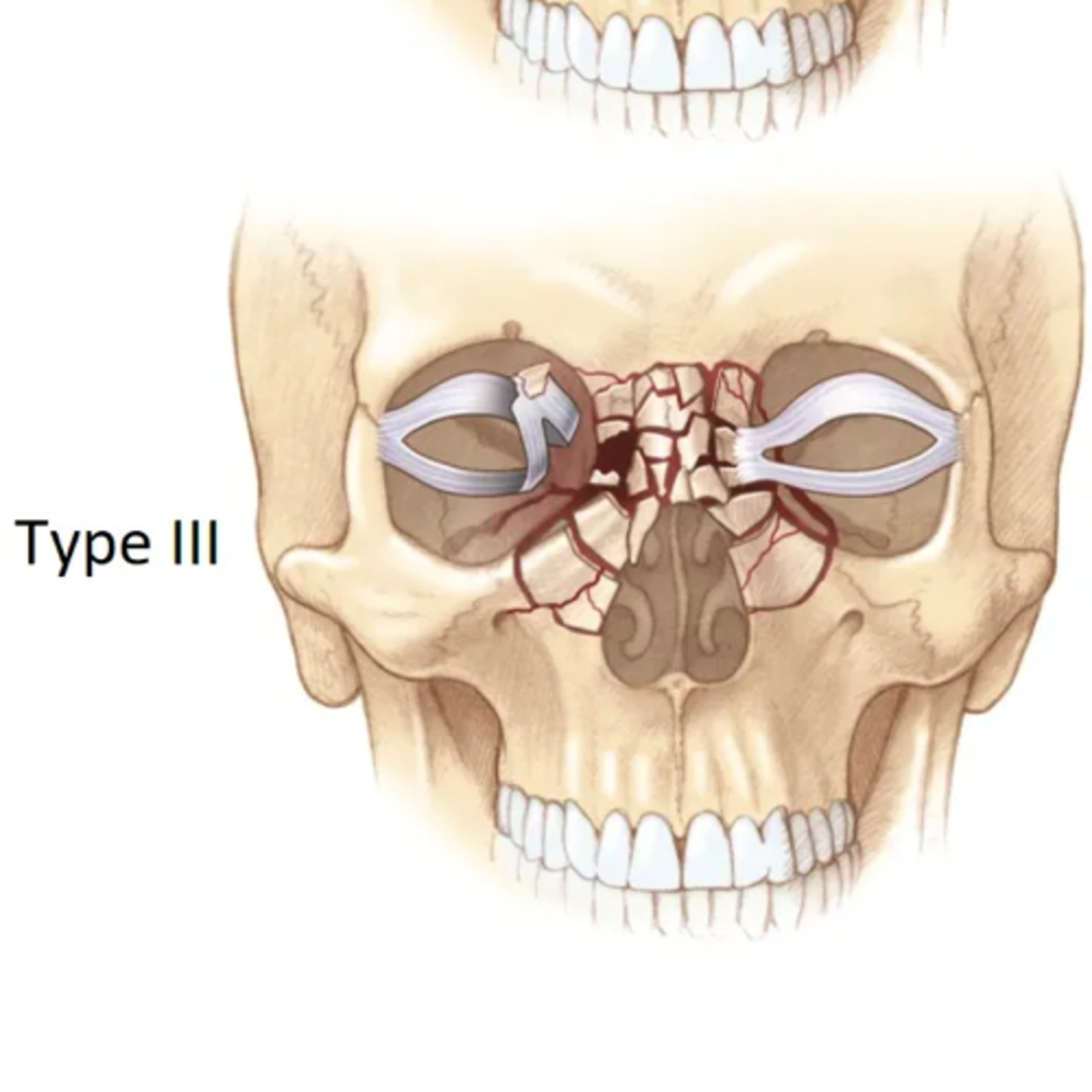
12.27.23 Quick Review #86 - #trauma #facialtrauma #NOE #fracture #facialfracture #ENT #plasticsurgery #doctorgallagher #oralsurgery #oralsurgeon #dentist #dentistry #dental The Markowitz and Manson classification system for naso-orbitoethmoid (NOE) fractures categorizes these fractures into 3 types: 1. Type I: The medial canthal tendon is intact and connected to a single, central fracture fragment. This type indicates less severe injury. 2. Type II: The fracture is comminuted, but the medial canthal tendon remains attached to a single bone fragment. 3. Type III: Comminution extends to the medial canthal tendon insertion site on the anterior medial orbital wall at the level of the lacrimal fossa, resulting in avulsion of the tendon. This is the most severe type. The surgical technique for repairing NOE fractures typically involves: 1. Incision and Exposure: A surgical incision is made to adequately expose the fracture site. This often involves a bicoronal or transconjunctival approach for better visualization. 2. Reduction of Fracture: • Types I & II: The large fracture fragment, to which the medial canthal tendon is attached, is carefully repositioned to its original anatomical location. • Type III: Stabilizing the comminuted bony fragments with miniplates and screws, paying special attention to the area of the medial canthal tendon. Precise reattachment of the medial canthal tendon is crucial, often requiring specialized techniques like transnasal wiring or drill hole canthopexy. 3. Fixation: The fracture is then stabilized using appropriate fixation techniques, which might include miniplates or screws, ensuring that the medial canthal tendon remains properly aligned. 4. Closure: Finally, the incision is closed with careful attention to avoid any tension on the skin and soft tissues, reducing the risk of postoperative complications. References: 1. Hacking, C., Deng, F., & Weerakkody, Y. (2021). Markowitz and Manson classification system of naso-orbitoethmoid fractures. Radiopaedia.org. Retrieved December 27, 2023, from https://lnkd.in/eaM_ehAP 2. Markowitz, B. L., Manson, P. N., Sargent, L., et al. (1991). Management of the medial canthal tendon in nasoethmoid orbital fractures: the importance of the central fragment in classification and treatment. Plastic and Reconstructive Surgery, 87(5), 843-853. 3. Manson, P. N., Markowitz, B., Mirvis, S., Dunham, M., & Yaremchuk, M. (1985). Toward CT-based facial fracture treatment. Plastic and Reconstructive Surgery, 75(6), 781-791. 4. Abubaker, A.O., Lam, D., & Benson, K. (2016). OMFS Secrets (3rd ed.). Elsevier. 5. ChatGPT. 2023.
What this episode covers
12.27.23 Quick Review #86 - #trauma #facialtrauma #NOE #fracture #facialfracture #ENT #plasticsurgery #doctorgallagher #oralsurgery #oralsurgeon #dentist #dentistry #dental The Markowitz and Manson classification system for naso-orbitoethmoid (NOE) fractures categorizes these fractures into 3 types: 1. Type I: The medial canthal tendon is intact and connected to a single, central fracture fragment. This type indicates less severe injury. 2. Type II: The fracture is comminuted, but the medial canthal tendon remains attached to a single bone fragment. 3. Type III: Comminution extends to the medial canthal tendon insertion site on the anterior medial orbital wall at the level of the lacrimal fossa, resulting in avulsion of the tendon. This is the most severe type. The surgical technique for repairing NOE fractures typically involves: 1. Incision and Exposure: A surgical incision is made to adequately expose the fracture site. This often involves a bicoronal or transconjunctival approach for better visualization. 2. Reduction of Fracture: • Types I & II: The large fracture fragment, to which the medial canthal tendon is attached, is carefully repositioned to its original anatomical location. • Type III: Stabilizing the comminuted bony fragments with miniplates and screws, paying special attention to the area of the medial canthal tendon. Precise reattachment of the medial canthal tendon is crucial, often requiring specialized techniques like transnasal wiring or drill hole canthopexy. 3. Fixation: The fracture is then stabilized using appropriate fixation techniques, which might include miniplates or screws, ensuring that the medial canthal tendon remains properly aligned. 4. Closure: Finally, the incision is closed with careful attention to avoid any tension on the skin and soft tissues, reducing the risk of postoperative complications. References: 1. Hacking, C., Deng, F., & Weerakkody, Y. (2021). Markowitz and Manson classification system of naso-orbitoethmoid fractures. Radiopaedia.org. Retrieved December 27, 2023, from https://lnkd.in/eaM_ehAP 2. Markowitz, B. L., Manson, P. N., Sargent, L., et al. (1991). Management of the medial canthal tendon in nasoethmoid orbital fractures: the importance of the central fragment in classification and treatment. Plastic and Reconstructive Surgery, 87(5), 843-853. 3. Manson, P. N., Markowitz, B., Mirvis, S., Dunham, M., & Yaremchuk, M. (1985). Toward CT-based facial fracture treatment. Plastic and Reconstructive Surgery, 75(6), 781-791. 4. Abubaker, A.O., Lam, D., & Benson, K. (2016). OMFS Secrets (3rd ed.). Elsevier. 5. ChatGPT. 2023.
NOW PLAYING
“What are the Types of NOE (Naso-orbitoethmoid) Fractures and How To Repair Them?”
No transcript for this episode yet
Similar Episodes
No similar episodes found.
Similar Podcasts
No similar podcasts found.