EPISODE · Jun 17, 2024 · 3 MIN
“What Is ‘Rigid’ vs. ‘Non-Rigid’ Fixation?”
from Dr. Gallagher's Podcast · host Brendan Gallagher, DDS
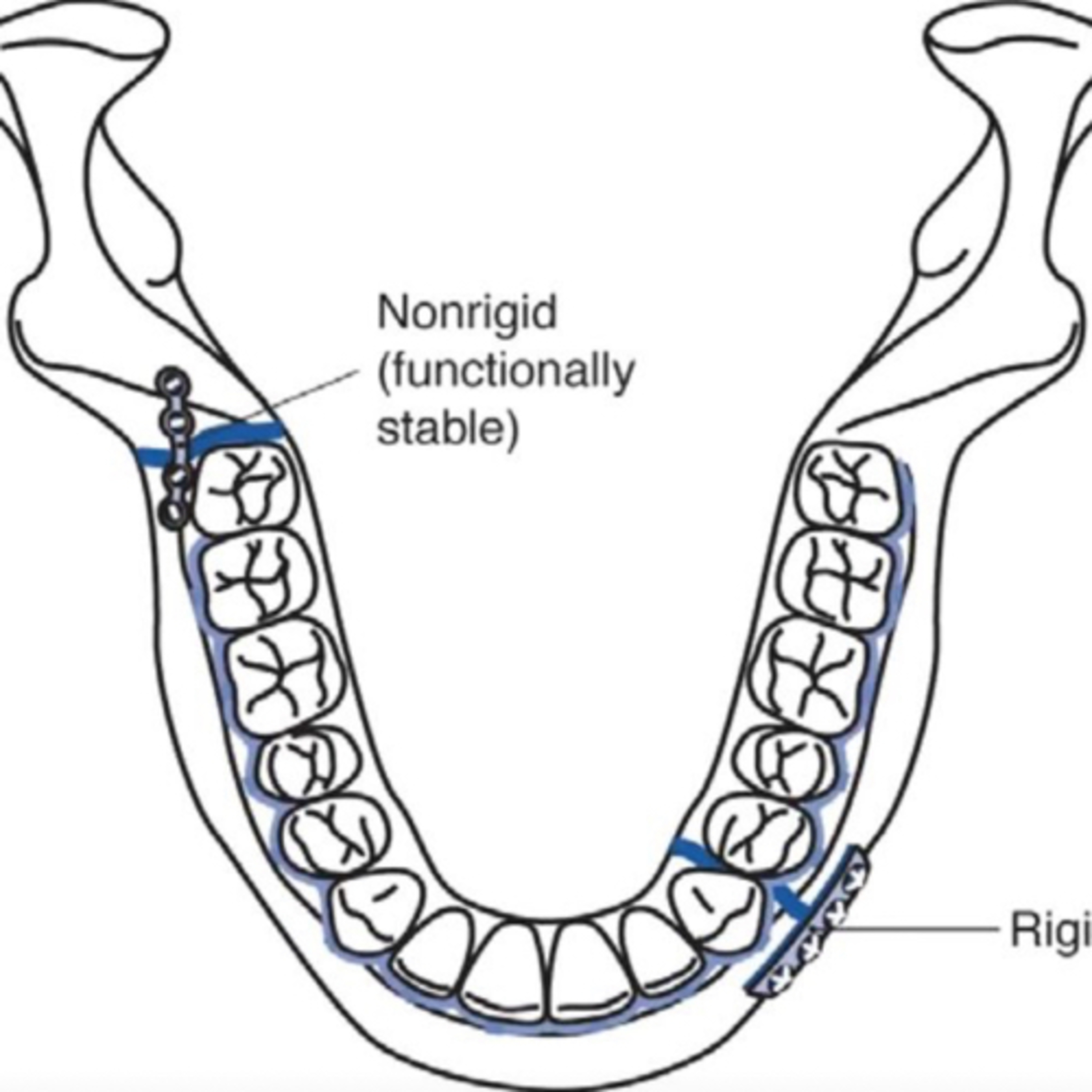
6.17.24 Quick Review #151 - #surgery #surgeon #doctorgallagher #oralsurgery #oralsurgeon #omfs #dentist #dentistry #dental In the context of mandibular fracture repair, “rigid” and “non-rigid” fixation refer to different techniques used to stabilize the fractured bone segments: Rigid Fixation: Rigid fixation involves the use of plates and screws to hold the fractured segments of the mandible firmly in place, preventing any movement between them. Techniques: • Commonly uses titanium plates and screws. • Plates can be placed either intraorally or extraorally. • Often requires more extensive surgical exposure. Advantages: • Provides stable fixation, allowing for immediate function and early mobilization. • Reduces the need for maxillomandibular fixation (MMF), which is often uncomfortable for patients. • Generally associated with lower rates of malunion and nonunion. • Allows for more predictable and precise anatomical reduction. Disadvantages: • More invasive, potentially leading to increased surgical time and risk of complications. • Higher cost due to the materials and techniques used. Indications: • Used in more complex or comminuted fractures. • Indicated in fractures where precise anatomical alignment is crucial. • Preferred in situations where early function is desired. Non-Rigid Fixation: Non-rigid fixation typically involves the use of wires, arch bars, or other devices that allow for some movement between the fractured segments. Techniques: • Common methods include intermaxillary fixation (IMF) using wires or arch bars. • Less invasive than rigid fixation techniques. • Often performed intraorally. Advantages: • Simpler and less invasive, usually resulting in shorter surgical time. • Lower cost compared to rigid fixation. • Suitable for less complex fractures. Disadvantages: • Generally requires prolonged MMF, which can be uncomfortable for the patient. • Limited stability compared to rigid fixation, potentially leading to higher rates of malunion or nonunion. • Patients may need to be on a liquid diet for an extended period. Indications: • Used for simple fractures, especially those with favorable fracture lines. • Suitable for children or patients with less complex fractures. • Often employed in resource-limited settings or when rigid fixation is not feasible. Summary • Rigid Fixation: More stable, allows early function, suitable for complex fractures, but is more invasive and costly. • Non-Rigid Fixation: Simpler, less invasive, suitable for less complex fractures, but usually requires longer MMF and provides less stability. References: 1. Ellis, E. (2022). Rigid versus nonrigid fixation. In M. Miloro, G. E. Ghali, P. E. Larsen, & P. Waite (Eds.), Peterson’s Principles of Oral and Maxillofacial Surgery (4th ed., pp. 539-554). Springer. 2. Fonseca, R. J., Barber, H. D., Powers, M. P., & Frost, D. E. (2000). Oral and Maxillofacial Trauma (2nd ed.). W.B. Saunders Company. 3. ChatGPT. 2024. - #podcast #podcasts #dentalpodcast #dentalpodcasts #doctorgallagherpodcast #doctorgallagherspodcast #doctor #dentistry #oralsurgery #dental #viral #dentalschool #dentalstudent #omfs #surgeon #doctorlife #dentistlife #residency #oralsurgeon #dentist #doctorgallagher
What this episode covers
6.17.24 Quick Review #151 - #surgery #surgeon #doctorgallagher #oralsurgery #oralsurgeon #omfs #dentist #dentistry #dental In the context of mandibular fracture repair, “rigid” and “non-rigid” fixation refer to different techniques used to stabilize the fractured bone segments: Rigid Fixation: Rigid fixation involves the use of plates and screws to hold the fractured segments of the mandible firmly in place, preventing any movement between them. Techniques: • Commonly uses titanium plates and screws. • Plates can be placed either intraorally or extraorally. • Often requires more extensive surgical exposure. Advantages: • Provides stable fixation, allowing for immediate function and early mobilization. • Reduces the need for maxillomandibular fixation (MMF), which is often uncomfortable for patients. • Generally associated with lower rates of malunion and nonunion. • Allows for more predictable and precise anatomical reduction. Disadvantages: • More invasive, potentially leading to increased surgical time and risk of complications. • Higher cost due to the materials and techniques used. Indications: • Used in more complex or comminuted fractures. • Indicated in fractures where precise anatomical alignment is crucial. • Preferred in situations where early function is desired. Non-Rigid Fixation: Non-rigid fixation typically involves the use of wires, arch bars, or other devices that allow for some movement between the fractured segments. Techniques: • Common methods include intermaxillary fixation (IMF) using wires or arch bars. • Less invasive than rigid fixation techniques. • Often performed intraorally. Advantages: • Simpler and less invasive, usually resulting in shorter surgical time. • Lower cost compared to rigid fixation. • Suitable for less complex fractures. Disadvantages: • Generally requires prolonged MMF, which can be uncomfortable for the patient. • Limited stability compared to rigid fixation, potentially leading to higher rates of malunion or nonunion. • Patients may need to be on a liquid diet for an extended period. Indications: • Used for simple fractures, especially those with favorable fracture lines. • Suitable for children or patients with less complex fractures. • Often employed in resource-limited settings or when rigid fixation is not feasible. Summary • Rigid Fixation: More stable, allows early function, suitable for complex fractures, but is more invasive and costly. • Non-Rigid Fixation: Simpler, less invasive, suitable for less complex fractures, but usually requires longer MMF and provides less stability. References: 1. Ellis, E. (2022). Rigid versus nonrigid fixation. In M. Miloro, G. E. Ghali, P. E. Larsen, & P. Waite (Eds.), Peterson’s Principles of Oral and Maxillofacial Surgery (4th ed., pp. 539-554). Springer. 2. Fonseca, R. J., Barber, H. D., Powers, M. P., & Frost, D. E. (2000). Oral and Maxillofacial Trauma (2nd ed.). W.B. Saunders Company. 3. ChatGPT. 2024. - #podcast #podcasts #dentalpodcast #dentalpodcasts #doctorgallagherpodcast #doctorgallagherspodcast #doctor #dentistry #oralsurgery #dental #viral #dentalschool #dentalstudent #omfs #surgeon #doctorlife #dentistlife #residency #oralsurgeon #dentist #doctorgallagher
NOW PLAYING
“What Is ‘Rigid’ vs. ‘Non-Rigid’ Fixation?”
No transcript for this episode yet
Similar Episodes
Dec 5, 2025 ·50m
Oct 9, 2025 ·33m
Oct 3, 2025 ·40m
Sep 11, 2025 ·31m
Aug 27, 2025 ·39m
Aug 18, 2025 ·54m