EPISODE · Mar 28, 2026 · 21 MIN
Racial Disparities in Cesarean Section Rates
from Culture Coalition Podcast
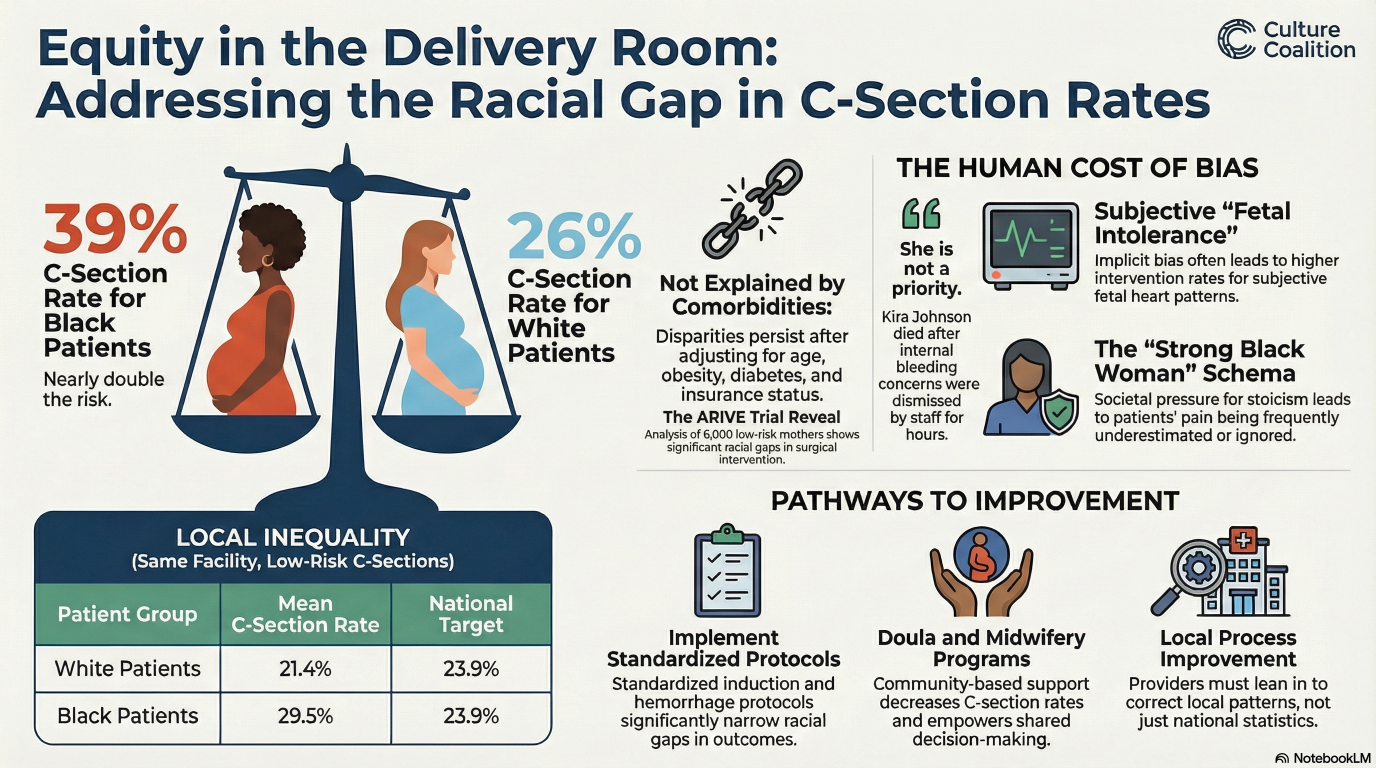
Beyond the Chart: Why Clinical Risk Factors Don’t Explain the Black-White C-Section GapThe Myth of the "High-Risk" Patient Many clinicians assume Black-White C-section disparities stem from higher comorbidity rates like obesity or hypertension. However, research proves these gaps persist even when medical histories are identical. As advocates, we must acknowledge that adjusting for age and BMI does not erase the divide. The "high-risk patient" narrative is a myth; the real risk lies within systemic practice patterns.It’s Not the Comorbidities: The Data Speaks Large-scale data confirms that clinical risk factors fail to explain the divide. A 2025 JAMA study found that after risk-adjusting for hypertension and BMI, Black patients still faced a significantly higher risk: an Adjusted Risk Ratio (ARR) of 1.23 for nulliparous patients and 1.33 for multiparous individuals without a prior cesarean. A California population study concluded:"The lack of difference in facility or patient characteristics between hospitals with low cesarean delivery rates among Black patients and those with high rates suggests that unconscious bias and structural racism potentially play important roles."The Subjectivity Trap: When "Judgment Calls" Create Disparity Disparities are primarily driven by Physician Subjectivity in three areas: labor dystocia, fetal concern, and "no labor" (e.g., macrosomia). These "judgment calls" invite implicit bias and medical gaslighting. Providers often follow a "healthcare script" rooted in the false assumption of higher pain tolerance in Black patients, leading to the dismissal of symptoms. Remarkably, in hospitals meeting targets for White patients (mean 21.4%), the rate for Black patients remained 29.5%.The Clinical Lifeline: Shared Decision-Making and Doula Support. To mitigate bias, we must implement objective guardrails. Doula care serves as a Clinical Lifeline, providing continuous support that evidence shows reduces primary C-sections. Standardized protocols—such as Shared Decision-Making (SDM) tools, "Pitocin Checklists," and "Pause for the Cause" algorithms for Category II Fetal Heart Tracings (FHTs)—replace subjective impressions with data-driven management. These tools protect patients from gaslighting by ensuring clinical evidence, not bias, dictates intervention.Conclusion: From National Crisis to Local Progress Closing this gap is a population-based necessity and a local process improvement priority. We must replace biased clinical scripts with standardized, inclusive care models that safeguard patient autonomy. If the clinical data doesn't justify the intervention, what part of our practice pattern does? Hosted on Acast. See acast.com/privacy for more information.
What this episode covers
Beyond the Chart: Why Clinical Risk Factors Don’t Explain the Black-White C-Section GapThe Myth of the "High-Risk" Patient Many clinicians assume Black-White C-section disparities stem from higher comorbidity rates like obesity or hypertension. However, research proves these gaps persist even when medical histories are identical. As advocates, we must acknowledge that adjusting for age and BMI does not erase the divide. The "high-risk patient" narrative is a myth; the real risk lies within systemic practice patterns.It’s Not the Comorbidities: The Data Speaks Large-scale data confirms that clinical risk factors fail to explain the divide. A 2025 JAMA study found that after risk-adjusting for hypertension and BMI, Black patients still faced a significantly higher risk: an Adjusted Risk Ratio (ARR) of 1.23 for nulliparous patients and 1.33 for multiparous individuals without a prior cesarean. A California population study concluded:"The lack of difference in facility or patient characteristics between hospitals with low cesarean delivery rates among Black patients and those with high rates suggests that unconscious bias and structural racism potentially play important roles."The Subjectivity Trap: When "Judgment Calls" Create Disparity Disparities are primarily driven by Physician Subjectivity in three areas: labor dystocia, fetal concern, and "no labor" (e.g., macrosomia). These "judgment calls" invite implicit bias and medical gaslighting. Providers often follow a "healthcare script" rooted in the false assumption of higher pain tolerance in Black patients, leading to the dismissal of symptoms. Remarkably, in hospitals meeting targets for White patients (mean 21.4%), the rate for Black patients remained 29.5%.The Clinical Lifeline: Shared Decision-Making and Doula Support. To mitigate bias, we must implement objective guardrails. Doula care serves as a Clinical Lifeline, providing continuous support that evidence shows reduces primary C-sections. Standardized protocols—such as Shared Decision-Making (SDM) tools, "Pitocin Checklists," and "Pause for the Cause" algorithms for Category II Fetal Heart Tracings (FHTs)—replace subjective impressions with data-driven management. These tools protect patients from gaslighting by ensuring clinical evidence, not bias, dictates intervention.Conclusion: From National Crisis to Local Progress Closing this gap is a population-based necessity and a local process improvement priority. We must replace biased clinical scripts with standardized, inclusive care models that safeguard patient autonomy. If the clinical data doesn't justify the intervention, what part of our practice pattern does? Hosted on Acast. See acast.com/privacy for more information.
NOW PLAYING
Racial Disparities in Cesarean Section Rates
No transcript for this episode yet
Similar Episodes
Mar 26, 2026 ·1m
Jan 2, 2026 ·47m
Dec 21, 2025 ·46m